GMC says
A letter I wrote this morning to the world’s first medical defence organisation that is proud of its rich history of guiding, supporting and defending its members:
Dear Medical Defence Union,
Here, I speak more as the mother of a deceased child than as a Consultant Anaesthetist. When a patient comes to my hospital to have surgery, there is a legal contract between him/her and the hospital. As per that, the hospital is obliged to safely complete his/her operation.
When I see that patient on the morning of their surgery, I speak with them and gain their confidence. The trust they place in me when I look into their eyes and assure them safety is not legislated for. Trust is an empowering human sentiment essential to the patient, enabling them to come for their operation. Trust is the basis of any meaningful relationship.
2 days before my son died, his GP, Dr F assured us that he was on the right medications and would soon start showing signs of improvement. After my 20 year old son, Saagar Naresh’s death on the 16th of October 2014, I didn’t hear at all from our GP. Not a word of condolence or sympathy. Complete silence. At the Coroner’s court the GP said that he followed the advice given to him by the MDU, to not call me after my son’s death.
Considering he knew me for 10 years and I entrusted my child’s well-being in his hands, I think it would have been ‘basic decency’ for him to call or visit. Legally speaking, a 20 year old is not a child. But for me he is. Human relationships are way beyond ‘legal’.
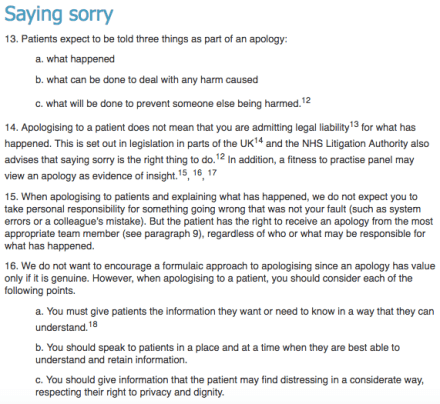
In light of GMC’s Duty of Candour, please rethink your advice in the future. The practice of medicine is founded on humanity.
Please do not take it away.
Kind regards,
SM.