“What can we do to offer wrap-around care to our patients?”
In the live Q&A at the end of the NCISH conference yesterday, this question was asked of the panel. The Chairperson directed it towards me. I can’t remember what I said. This morning I woke up with what I would have liked to say.
For wrapping, we need two things. One, the fabric which we are going to use to wrap and the person we want to wrap. Let’s discuss them one by one.
- The fabric
The fabric of Suicide prevention in Health-Care is made up of two things – people and systems. Let’s look at them a bit closely.
- People
What are the beliefs of the people?
I know of an ENT surgeon from another country who wanted to move to the UK and the only job he could find was in Psychiatry. So, he is now training to be a Psychiatrist. Is he interested in suicide prevention? Do Health-care professionals believe that suicides are preventable? Are they content that simply by treating mental illness they are doing their job?
What are the attitudes and abilities of the people?
When the Emergency department calls to say there is a suicidal individual waiting to be seen, how do they feel? Are they excited to have an opportunity to make a difference? Or is it a drain on the limited time and energy they have? Do they know how to build a compassionate connection with someone who has lost all hope? Have they received any training in Suicide Prevention? Do they have enough self-compassion to look after someone else well?
Do they have the resources and the knowledge to do a good job?
Do they have access to their past history? Do they have beds on the ward? Can they ask a colleague for a second opinion if they have a doubt about how to involve family or friends in their care? Do they know of other resources, like charities, activities and people that may help this person? Do they have comprehensive and informative leaflet they can share with them? Do they have the means to follow them up?
b. Systems
Does the system have capacity? Are the various parts of the system effective and joint-up enough to be able to hold the person they are trying to wrap or are there big holes in this part of the fabric? Do the various parts of the system share the same mental model, a shared knowledge, pre-suppositions, and beliefs that can be used to help achieve mutual goals? Are their practices evidence- based? Do they investigate deaths with a view to learn lessons and implement change? Do they look after the well-being and emotional health of their employees? Do they hold themselves accountable when things go wrong?
2. The person
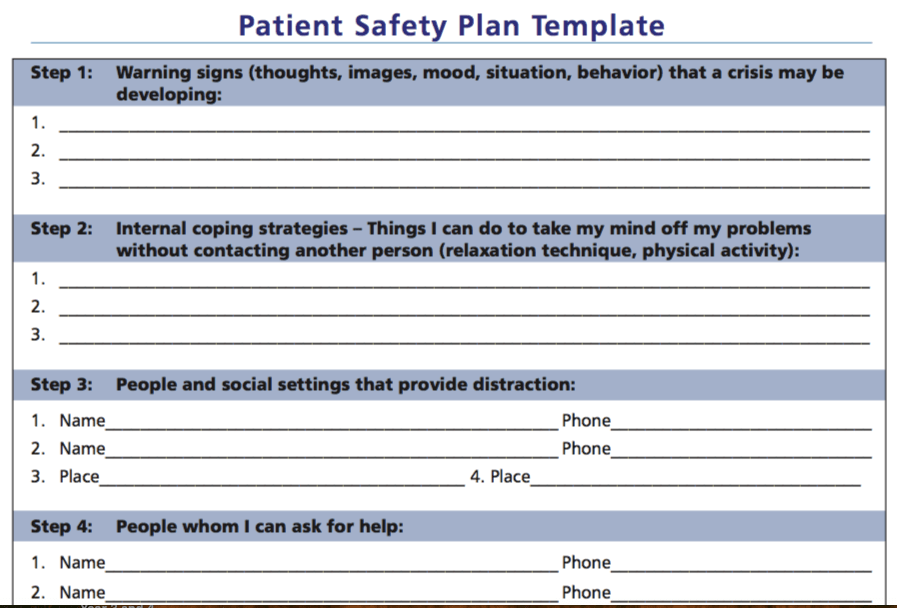
Allowing space for them to express themselves. Help maintain their sense of agency. Inform them it is safer for them to involve other people who care for them. Equip them with resources. Give them the support they need. Ask them what would help them? Listen. Sit with their despair. Acknowledge it. Keep them connected with their life as they know it. Keep hope alive for them.
Know that the person at the centre of the wrapping is of great value.
Information is useful if it becomes knowledge. Knowledge is useful when it becomes wisdom. So, let us not stop at information.
Ref:
Reaching common ground: The role of shared mental models in patient safety : https://journals.sagepub.com/doi/full/10.1177/2516043518805326